Ellen’s recent hip issues have brought the subject of hip pain and degeneration to the forefront of our attention. She is likely looking at needing a hip replacement surgery. Why? Hip replacement surgery is now among the most commonly performed orthopedic procedures in the developed world. Yet in hunter-gatherer populations and traditional cultures, severe hip degeneration is remarkably rare. Something about modern life is destroying our hips — and it starts long before any pain begins.
likely looking at needing a hip replacement surgery. Why? Hip replacement surgery is now among the most commonly performed orthopedic procedures in the developed world. Yet in hunter-gatherer populations and traditional cultures, severe hip degeneration is remarkably rare. Something about modern life is destroying our hips — and it starts long before any pain begins.
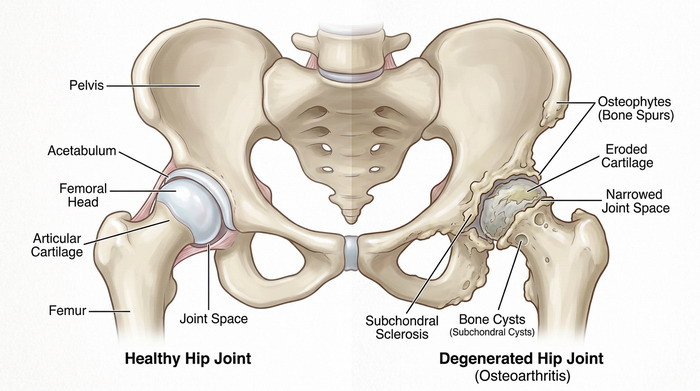
The hip has a genuine anatomical vulnerability: a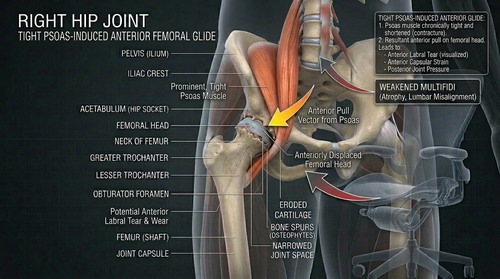 deep ball-and-socket design that concentrates load on a small area of cartilage, dependent on surrounding muscles for protection and on rhythmic movement for its very nutrition. In a body that moves freely and often, this design works beautifully. In a body shaped by chairs, flat floors, and chronic inactivity, it becomes a slow-motion failure.
deep ball-and-socket design that concentrates load on a small area of cartilage, dependent on surrounding muscles for protection and on rhythmic movement for its very nutrition. In a body that moves freely and often, this design works beautifully. In a body shaped by chairs, flat floors, and chronic inactivity, it becomes a slow-motion failure.
The chair problem
The single most underappreciated cause of hip dege neration is the chair. Prolonged sitting does two damaging things simultaneously. It allows the hip flexor muscles — particularly the psoas, which runs from the lumbar spine across the front of the hip — to adaptively shorten and tighten. And it progressively weakens the deep spinal stabilizers, especially the multifidi, which run along the lower back and keep the lumbar vertebrae properly aligned.
neration is the chair. Prolonged sitting does two damaging things simultaneously. It allows the hip flexor muscles — particularly the psoas, which runs from the lumbar spine across the front of the hip — to adaptively shorten and tighten. And it progressively weakens the deep spinal stabilizers, especially the multifidi, which run along the lower back and keep the lumbar vertebrae properly aligned.
When the multifidi weaken, the spine loses its segmental stability. The psoas — now pressed into service as a spinal prop — becomes chronically overactive, never truly switching off. This creates a constant, low-grade compression of the femoral head (the ball of the hip) into the acetabulum (the socket), disrupting the rhythmic loading and unloading that cartilage depends on for its nutrient supply. Cartilage has no blood vessels. It feeds itself through movement. Take that movement away, and cartilage quietly starves.
How a tilted pelvis damages the joint
The tight, overactive psoas also pulls the pelvis int o an anterior tilt — tipping it forward, exaggerating the lumbar curve, and shifting the femoral head toward the front of the socket. This matters because the anterior acetabulum has thinner, more fragile cartilage than the load-bearing dome at the top. Over the years, this mismatch concentrates force precisely where the joint is least equipped to handle it.
o an anterior tilt — tipping it forward, exaggerating the lumbar curve, and shifting the femoral head toward the front of the socket. This matters because the anterior acetabulum has thinner, more fragile cartilage than the load-bearing dome at the top. Over the years, this mismatch concentrates force precisely where the joint is least equipped to handle it.
The body compensates predictably. Without proper hip extension in late stance — the moment when the leg drives b ehind you as you walk — the lumbar spine hyperextends instead, loading the lower back and reinforcing the very muscle imbalances driving the problem. The gluteal muscles, which should be the primary hip stabilizers, grow progressively weaker with disuse, placing even greater demand on the hip joint itself.
ehind you as you walk — the lumbar spine hyperextends instead, loading the lower back and reinforcing the very muscle imbalances driving the problem. The gluteal muscles, which should be the primary hip stabilizers, grow progressively weaker with disuse, placing even greater demand on the hip joint itself.
“In traditional cultures that squat, kneel, and move through wide ranges of motion daily, hip osteoarthritis is uncommon. We largely invented the condition along with the office chair.”
Why do the multifidi matter so much?
The multifidi are not large, powerful muscles. They a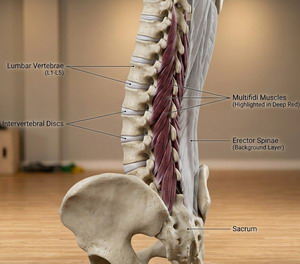 re small, segmental stabilizers whose job is to resist unwanted movement between individual vertebrae — the fine-grained, moment-to-moment control that keeps the spine honest. When they atrophy (which happens rapidly and often asymmetrically after even a single episode of back pain), the larger global muscles — the psoas, erector spinae, quadratus lumborum — have to work harder to compensate. The result is a chronically braced, compressed spine sitting on a tilted pelvis, with an overworked hip joint caught in the middle.
re small, segmental stabilizers whose job is to resist unwanted movement between individual vertebrae — the fine-grained, moment-to-moment control that keeps the spine honest. When they atrophy (which happens rapidly and often asymmetrically after even a single episode of back pain), the larger global muscles — the psoas, erector spinae, quadratus lumborum — have to work harder to compensate. The result is a chronically braced, compressed spine sitting on a tilted pelvis, with an overworked hip joint caught in the middle.
Crucially, research shows that multifidus atrophy does not spontaneously reverse, even when pain resolves, and a person returns to normal activity, including heavy exercise. The muscle needs to be specifically re-recruited before it can meaningfully contribute to any other movement, which is why the order of rehabilitation matters as much as the exercises themselves.
A three-phase path to recovery
Understanding this helps explain why different rehabilitation approaches suit different stages of the problem. Effective recovery generally follows a logical sequence:
The rehabilitation sequence
Phase 1: Reactivation
Restore neural recruitment of the multifidi and deep stabilizers before loading the spine in any direction.
Phase 2: Integration
Train the full posterior chain in coordinated patterns — hip hinging, sustained postures, pelvic anchoring.
Phase 3: Loading
Progressive strengthening through compound movements that challenge the whole system under increasing load.
Each exercise has a video link – click the exercise name.
Exercises by phase
Phase 1 — reactivation
Extend opposite arm and leg from hands and knee s, holding the lumbar spine completely still. The goal here is not muscle fatigue — it is restoring the nervous system’s ability to activate the deep stabilizers at all. 3 × 10 each side, slowly.
s, holding the lumbar spine completely still. The goal here is not muscle fatigue — it is restoring the nervous system’s ability to activate the deep stabilizers at all. 3 × 10 each side, slowly.
Phase 1 — reactivation

Lying on your back, drive your hips toward the ceiling with deliberate glute contraction. Begins restoring the posterior chain connection lost to prolonged sitting. Progress to single-leg once both sides feel equal.
Phase 2 — integration
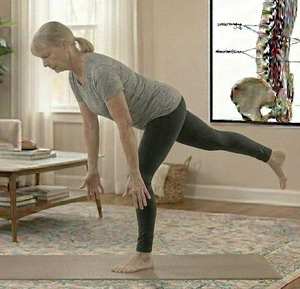
The Founder (Foundation Training)
A sustained hip hinge with arms extended and the s pine braced long. Trains the entire posterior chain at effective length — hamstrings, glutes, deep lumbar extensors — through isometric tension. Begin shallowly and only deepen as pelvic anchoring is established.
pine braced long. Trains the entire posterior chain at effective length — hamstrings, glutes, deep lumbar extensors — through isometric tension. Begin shallowly and only deepen as pelvic anchoring is established.
Phase 2 — integration
Sit with both legs bent at 90°, one in front, one to the side. Targets the hip capsule and psoas without stressing the lower back. Address hip flexor length only after stabilizer recruitment is underway.
side. Targets the hip capsule and psoas without stressing the lower back. Address hip flexor length only after stabilizer recruitment is underway.
Phase 2 — integration

Half-kneeling, tuck the pelvis under (posterior tilt) before leaning forward. The pelvic tuck is essential — without it, the lumbar spine simply extends, and the psoas remains unstretched.
Phase 2 — integration
Hip CARs
Slow, deliberate, controlled articular rotations of the hip joint through its full range. Maintains joint health, nourishes cartilage, and signals to the nervous system that the full range is actively usable.
Phase 3 — loading
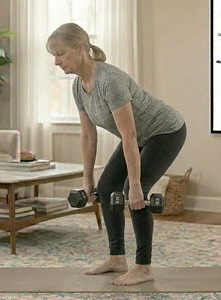
A hip hinge under load. Once posterior chain patterning is established, this drives genuine hypertrophy of the multifidi and surrounding musculature in a way that low-load exercises cannot. Start light and prioritize form.
Phase 3 — loading
Adds hip stability challenge under load. Rebuilds abductor strength that reduces joint reaction forces with every step you take, directly protecting the hip cartilage long-term.
Daily habit
Hanging in a relaxed deep squat for 1–2 minutes daily  restores hip range of motion and nourishes cartilage through cyclical loading. Traditional cultures maintain this position effortlessly throughout life — we have simply forgotten it.
restores hip range of motion and nourishes cartilage through cyclical loading. Traditional cultures maintain this position effortlessly throughout life — we have simply forgotten it.
Daily habit
Walking on varied terrain
Uneven ground activates hip stabilizers that flat surfaces never challenge. Even 20 minutes on a trail or grass makes a meaningful cumulative difference over time.
An important caution about sequencing
One of the most common rehabilitation mistakes i s skipping Phase 1 and going straight to loaded compound exercises. If the multifidi and deep stabilizers are neurologically inhibited — as they commonly are after pain or prolonged disuse — the global muscles simply compensate again during deadlifts and squats, reinforcing the very patterns causing harm. You cannot effectively load a muscle that the nervous system is not yet willing to activate.
s skipping Phase 1 and going straight to loaded compound exercises. If the multifidi and deep stabilizers are neurologically inhibited — as they commonly are after pain or prolonged disuse — the global muscles simply compensate again during deadlifts and squats, reinforcing the very patterns causing harm. You cannot effectively load a muscle that the nervous system is not yet willing to activate.
For patients with anterior pelvic tilt: Foundation Training’s posterior chain exercises are excellent, but the Fo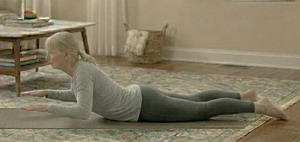 under and similar postures involve deliberate lumbar extension under load. This is safe and beneficial once pelvic anchoring is established — but in patients with a marked existing anterior tilt, close attention to adductor engagement and lower abdominal co-contraction is essential in early sessions. Done correctly, the exercise corrects the pattern; done without that anchoring, it can temporarily reinforce it.
under and similar postures involve deliberate lumbar extension under load. This is safe and beneficial once pelvic anchoring is established — but in patients with a marked existing anterior tilt, close attention to adductor engagement and lower abdominal co-contraction is essential in early sessions. Done correctly, the exercise corrects the pattern; done without that anchoring, it can temporarily reinforce it.
The habits that matter between sessions
Exercise is important, but the hours between sessio ns matter equally. Break sitting every 30–45 minutes with even a brief stand or walk. Consider working at a standing desk for part of the day, or spending time sitting on the floor, which forces constant small positional adjustments that chairs eliminate. Barefoot time on varied surfaces, even indoors, re-engages the foot and hip stabilizers that conventional footwear tends to suppress over time.
ns matter equally. Break sitting every 30–45 minutes with even a brief stand or walk. Consider working at a standing desk for part of the day, or spending time sitting on the floor, which forces constant small positional adjustments that chairs eliminate. Barefoot time on varied surfaces, even indoors, re-engages the foot and hip stabilizers that conventional footwear tends to suppress over time.
Excess body weight meaningfully increases the joint reaction forces through the hip with every step. Where relevant, gradual weight management is among the highest-impact interventions available — not as an aesthetic consideration, but as a straightforward matter of reducing the mechanical load your cartilage must absorb across thousands of daily steps.
Hip degeneration is not simply an inevitable conseq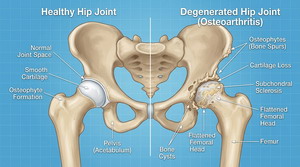 uence of aging. It is substantially a product of the postural and movement environment that modern life creates — and that means it is, in large part, within our power to prevent, slow, and, in early stages, reverse. The key is understanding the sequence: restore the nervous system’s access to the stabilizers first, then integrate them into whole-chain patterns, then load them progressively. Each stage enables the next.
uence of aging. It is substantially a product of the postural and movement environment that modern life creates — and that means it is, in large part, within our power to prevent, slow, and, in early stages, reverse. The key is understanding the sequence: restore the nervous system’s access to the stabilizers first, then integrate them into whole-chain patterns, then load them progressively. Each stage enables the next.
Take care,
David
Ellen
Success. Ellen finally has an appointment with an orth opedic doctor. The soonest they could get her in is not for another three weeks, but it is a step forward. Between now and then she needs to get some bloodwork. Ellen has slippery veins that don’t let go of their blood easily. To support the draw she works her arm out the day of the test and she loads up on electrolyte drinks to make the blood volume increase.
opedic doctor. The soonest they could get her in is not for another three weeks, but it is a step forward. Between now and then she needs to get some bloodwork. Ellen has slippery veins that don’t let go of their blood easily. To support the draw she works her arm out the day of the test and she loads up on electrolyte drinks to make the blood volume increase.
Scented indoor products – air pollution Indoor air scent products produce as much air pollution as automobiles. Breathing these nano sized particle ___________________________ “Our heads can gather and organize data, but it is our feelings that allow us to prioritize that data. “
~David DeLapp _____________________________________ Vitamin C may help prevent cancer Nitrates and nitrites form nitrosation products in th ____________________________ “People are driven, compelled subconsciously to recreate and repeat past traumatic or high drama experiences in an attempt to produce better results.“ ~David DeLapp ________________________________________ Eating eggs 5 times a week for Alzheimer’s A study of medicare claims has shown that those who ate eggs five times a week were 27% less likely to end up wi ________________________ “Attraction is based on our subconscious aligning with the other person in playing out a pattern that recreates old relationships that were unsatisfactory. We attempt to “win” at getting “our way” this time around.“ ~David DeLapp |


